

INTRODUCTION
Actinomycetes are those groups of bacteria which are thin and have cell wall made up of muramic acid. Their nuclei are prokaryotic and are susceptible to antibacterial antibiotics. They look similar to fungi superficially as they form branching filaments. They are related to mycobacteria and corynebacteria.

Image source: slideplayer
They are Gram-positive, non-sporing, non-motile, non-capsulated filaments. They break into bacillary and coccoid elements. They are also free living in nature and are mostly found in soil.
DIFFERENT GENERA OF ACTINOMYCETES
There are different genera of Actinomycetes that are of great medical importance. They are as follows.
- Anaerobic Actinomyces, Arachnia, Bifidobacterium and Rothia. Actinomyces is the major pathogenic form which is anaerobic or microaerophilic and non-acid fast.
- Aerobic Nocardia, Actinomadura, Dermatophilus and Streptomyces. Nocardia is aerobic and may be acid fast. Some Streptomyces species are related to diseases but are also a major source of antibiotics.
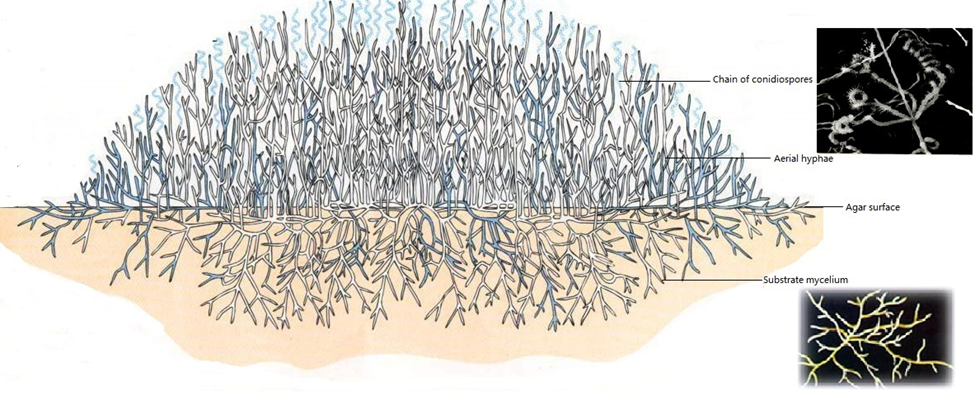
Image source: MDIS
HISTORY OF ACTINOMYCES
Actinomyces are the reason for lumpy jaw (actinomycosis) in cattle which seems like a mould-like organism. It was found by Bollinger in 1877. The name Actinomyces was coined by Harz which explains the ray-like appearance of the organism in the granules that characterize the lesions. For this Actinomyces are also called ray fungus. From human lesions also, Actinomyces were isolated as an anaerobic bacillus. This was done by Wolff and Israel in 1891. They also produced an experimental infection in some animals like rabbits and guinea pigs. Thus, the Actinomyces was named Actinomyces israelii. It was the reason of human actinomycosis. In cattle, actinomycosis is produced by Actinomyces bovis.
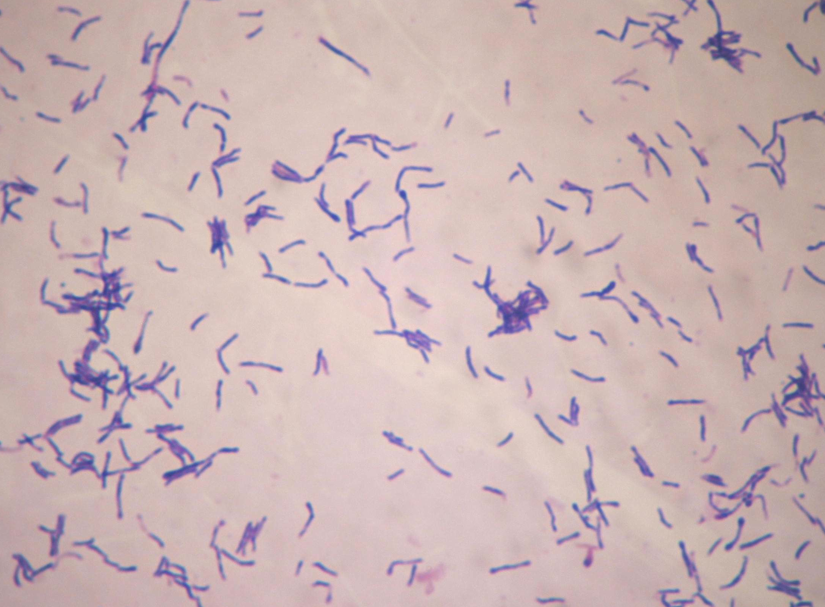
Image source: medlibes
WHAT IS ACTINOMYCOSIS?
Actinomycosis is a disease which is a chronic granulomatous infection. It is found both in human beings and animals. There is development of indurated swellings, mainly targeting the connective tissue, and also suppuration and the discharge of ‘sulphur granules’. The lesions often face towards the skin which may lead to multiple sinuses.
ACTINOMYCOSIS IN HUMAN BEINGS
It is an endogenous infection. The species of the causative agent are mostly found in mouth, intestine and vagina as a commensal. These organisms may invade other tissues in case of trauma, foreign bodies or poor oral hygiene. The common species as the causative agent is Actinomyces israelii. Some other species are also responsible for this disease condition. They are: A. naeslundii, A. viscosus, A. odontolyticum, A. meyeri, A. gerencsonei and Propionibacterium propionicum.
It is the mixed infection condition where other bacterial infections are also associated. This may increase the pathogenic effect.
OTHER BACTERIA ASSOCIATED WITH ACTINOMYCOSIS
Some of the bacteria associated with this disease condition are Bifidobacterium dentium, Actinobacillus actinomycetemcomitans, Eikenella corrodens, Haemophilus aphrophilus, bacteroides, fusobacteria, staphylococci and anaerobic streptococci.
CLINICAL FORMS OF ACTINOMYCOSIS
Actinomycosis is found in different clinical forms in human beings. They are:
1. Cervico-facial form
It is characterized by indurated lesions on the cheek and sub-maxillary regions.
2. Thoracic form
It is characterized by the presence of lesions in the lungs mainly pleura and pericardium which may spread outwards through the chest wall.
3. Abdominal form
It is characterized by presence of lesions around the cecum and may also involve the neighbouring tissues and the abdominal wall. Through portal vein the infection may reach to the liver which is exceptional.
4. Pelvic form
It is generally associated with the use of intrauterine devices. It is characterized by the formation of abscesses mostly in bone and soft tissue with chronic draining sinuses to the exterior.
SOME OTHER FORMS WHERE ACTINOMYCOSIS OCCURS
Actinomyces is also involved in gingivitis and periodontitis which are the inflammatory diseases of the gums and also sublingual plaques leading to root surface caries. It may also present as mycetoma.
In the exudate or secretion, sulphur granules are noticed. When observed in disease tissue, it is found as a long, branching mycelium with attached sulphur granules. If the bacterial species is to be isolated from clinical specimens, then, anaerobic environment must be maintained. In micro-aerophilic conditions also it can be identified and isolated. For treating this disease condition, surgical drainage or excision is performed along with the use of large doses of penicillin for several weeks or months.
WHAT IS THE LABORATORY DIAGNOSIS OF ACTINOMYCETES SPECIES?
1. Firstly, the sample like pus or tissue is collected. For pulmonary disease, sputum is required.
2. Gross examination of granules
- In pus, sulphur granules may be demonstrated by shaking it up in a test tube with some saline.
- When it is allowed to rest, the granules sediment and is withdrawn with the help of capillary pipette.
- Application of gauze pads over the discharging sinuses may also help to obtain the granules.
- Yellow or white colored granules ranging in size from minute specks to about 5 mm are observed.
3. Microscopy
- It is used to demonstrate the actinomycetes from the lesions or granules. They are observed under a cover slip.
- Gram stain is performed after they are crushed between the slides and then examined.
- The granules generally contain bacterial colonies which are found to consist of a dense network of thin, Gram-positive filaments.
- These are surrounded by a peripheral zone of swollen, radiating, club-shaped structures which give the appearance of sun ray.
- The clubs are believed to be antigen-antibody complexes.
4. Isolation in culture
- The granules of sulphur or pus with actinomycetes are washed and inoculated in thio-glycollate liquid medium.
- It can also be streaked on brain-heart infusion agar after which, are incubated anaerobically at 37 degree Celsius.
- Turbidity if demonstrated in thio-glycollate medium indicates the presence of Actinomycetes bovis.
- If fluffy balls are obtained at the bottom of the tube, it represents A. israelii.
- On solid media, small ‘spidery colonies’ in 48-72 hours if produced, also indicates A. israelii.
- These colonies if, left for 10 days, become large and heaped up with white and irregular or smooth form.
- Other species may show different forms of colonies.
5. Identification of species
- The isolate is then identified by microscopy, biochemical reactions and fluorescent antibody methods.
- Gel diffusion and immunofluorescence can differentiate A. israelii from other filamentous anaerobes that may produce granules in tissues.
HOW IS TREATMENT DONE?
For treating this disease condition, penicillin or tetracycline is used for long term only after which the response is achieved. The mentioned medicines should be used for several months which may be supplemented by surgery if necessary.
References:
i) https://www.hopkinsguides.com/hopkins/view/Johns_Hopkins_ABX_Guide/540005/all/Actinomyces
ii) https://www.britannica.com/science/actinomycete
iii) https://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-4-98