
Introduction
- Immunodeficiency diseases are condition where the defense mechanism of the body is impaired lading to repeated microbial infections of varying severity and sometimes enhanced susceptibility to malignancies.
- In this condition, the system fails to protect the host from disease causing agents or from malignant cells.
- Deficiency of defense mechanism may include:
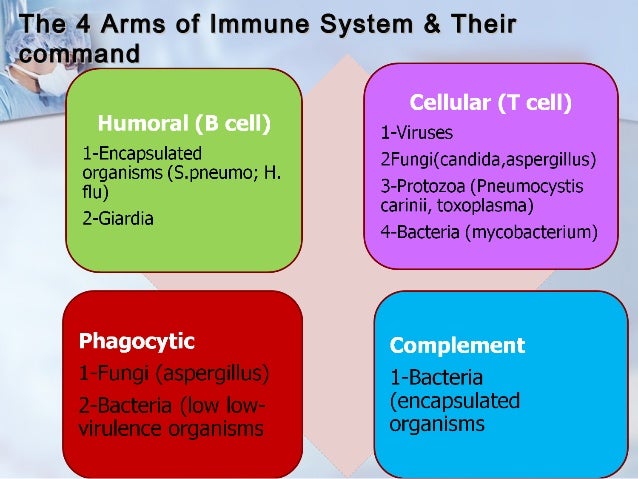
- Specific immune functions – humoral immunity, cell mediated immunity or both.
- Nonspecific immune functions –phagocytes, complement system which augment and act in conjunction with specific immune response.
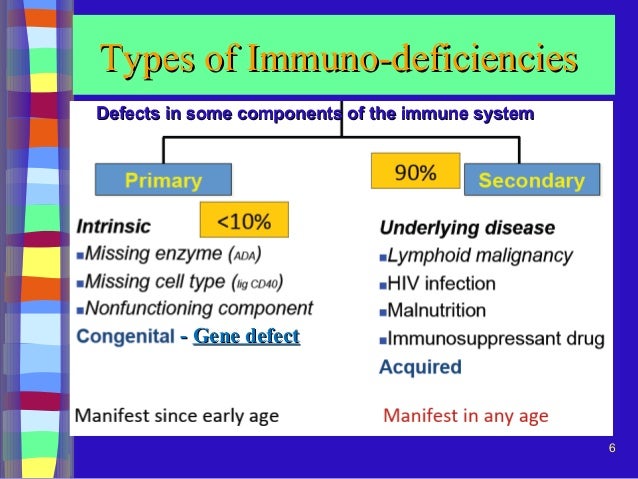
- Immunodeficiency are mainly of two types . They are:
A) Primary immunodeficiency/ genetic deficiency/ congenital deficiency
B) Secondary immunodeficiency/ acquired immunodeficiency
A) Primary immunodeficiency
- A condition resulting from a genetic or developmental defect of the immune system is called primary immunodeficiency.
- Most of the primary immunodeficiency are inherited thus called genetic deficiencies or congenital deficiencies.
- A primary immunodeficiency affects either adaptive or innate immune function.
- In adaptive immunodeficiency T cell, B cell or both components are involved whereas in innate immunodeficiency, phagocytes or complement factors are involved.
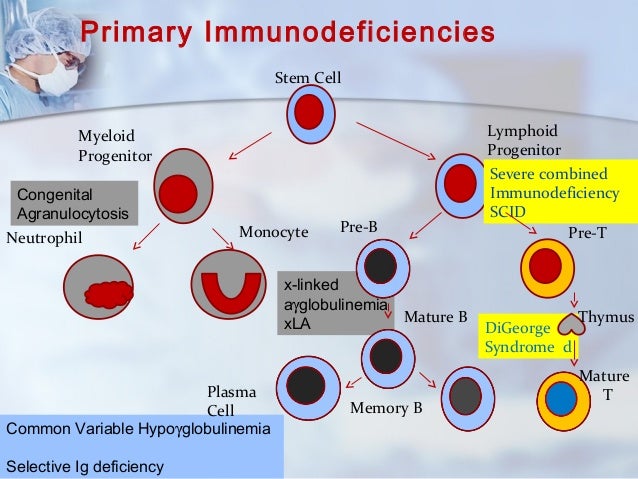
- Primary immunodeficiency can be categorized as:
a) Lymphoid immunodeficiency
b) Complement deficiency
c) Phagocytosis deficiency.
a) Lymphoid deficiency
- It may involve T cells, B cells or both.
- In B cells deficiency (Humoral deficiency), there appears complete absence of mature reticulating B cells, plasma cells and Ig.
- This type of disorder have diverse spectrum of disease.
- Patients with these disorders are usually subjected to recurrent bacterial infection but display normal immunity to most viral and fungal infections because the T cell branch of the immune system is largely unaffected.
- e.g., X-linked agammaglobulinemia, transient hypo hammaglobulinemia of infancy, common variable immunodeficiency, selective immunoglobulin deficiency, Transcobalamin II deficiency.
- In T cells (cellular deficiency), more severe and persistent infections are noticed than those of B cells defects.
- Deficiency of T cells is associated with abnormal antibody level because TH cells are involved in the generation and control of antibody synthesis.
- Abnormalities of T- lymphocyte development results in viral, intracellular bacterial, fungal and protozoan infection rather than acute bacterial infection.
- e.g., Thymic hypoplasia (Di George syndrome), chronic muco-cutaneous candidosis, purine nucleoside phopshorylase (PNP) deficiency.
- In combined immunodeficiency, both lineages are affected and are generally lethal.
- The onset of infection begins early in infancy and the prognosis from these infant causes early death unless therapeutic intervention reconstitutes their defective number of option.
- e.g.,Ataria telangiectasica, Wiskoh- Aldrich syndrome, Swis type agammaglobulinemia, etc.
b) Complement deficiency
- It results from the defect of complement system.
- It can be categorized as complement component deficiency and complement inhibitor deficiency.
- Complement components deficiency have been detected in genetic deficiencies in human.
- Genetic deficiencies of C10, C1γ, C1s, C4, and C2 component are associated with defects in activation of the classical pathway.
- This result in increased susceptibility to pyogenic infection.
- This may be transmitted as autosomal recessive traits.
- Hereditary agioneurotic edema is due to the genetic deficiency of C1.
- Deficiency of C3b in-activators has been associated with chronic recurrent pyogenic lesions.
- This may be transmitted as autosomal dominant trait.
- C3 deficiency results in defect of both classical and alternative pathways leading to pyogenic infection and in opsonization and phagocytosis.
- Deficiency of properdin factor results in impaired activation of alternative pathway that results in pyogenic infection.
c) Phagocytic deficiency
- It may be impaired by either intrinsic or extrinsic defects.
- Intrinsic disorders may be due to defects within the phagocytic cells such as enzyme deficiency.
- Extrinsic disorders may be due to deficiency of opsonin antibody, complement or other factors promoting phagocytosis or to the effects of drugs or anti-neutrophil auto-antibodies.
- Phagocytic dysfunction leads to increased susceptibility to infection ranging from mild recurrent skin infections to overwhelming systemic infection.
- e.g., chronic granulomatos disease, Job’s syndrome, etc.

B) Secondary immunodeficiency
- It is the loss of immune function which arises when infection, drugs (like immunosuppressive agents, corticosteroids), nutritional in-adequencies, metabolic disorders and malignancies lead to defects in specific and non-specific immunity.
- These are very common than primary immunodeficiency.
- Deficiencies of humoral and cellular immune responses may occur secondarily during the course of many diseases process.
- Various hormonal and metabolic disorders can also result in immune deficiency including anemia, hypothyroidism, diabetes and hypoglycemia.
- Smoking, alcoholism and drug abuse also depress immune response.
- The most well-known example of a secondary immune deficiency is the immunodeficiency caused by the human immunodeficiency virus, or HIV.
- HIV attacks certain cells in the immune system and prevents them from carrying out their proper functions against microbes.
- When the immune system is sufficiently weakened, infected people catch atypical and severe infections.
- This is then called the Acquired Immunodeficiency Syndrome, or AIDS. AIDS at this time is often treated by a specialized multidisciplinary team.


References:
i) https://www.healthline.com/health/immunodeficiency-disorders#types
ii) https://www.mayoclinic.org/diseases-conditions/primary-immunodeficiency/symptoms-causes/syc-20376905