

- The air entering the pleural cavity is the reason of pneumothorax.
- Negative pressure that exists between the visceral pleura (surrounding the lungs) and the parietal pleura (lining the thoracic cavity) allows the lungs to be filled by chest wall expansion normally.
- The pleural space contains only a few millilitres of lubricating fluid that helps to reduce friction when the tissues move.
- Partial or complete lungs collapse occurs when air enters this space which causes change to positive pressure.

- As the volume of air in the pleural space increases, the lungs volume decreases.
- This condition should be suspected if any trauma occurs in the chest wall.
- Pneumothorax is classified as open (air entering through an opening in the chest wall) or closed (no external wound).
- Mild tachycardia and dyspnea are the manifestations in a small pneumothorax.
- There is presence of respiratory distress including shallow, rapid respiration, dyspnea, air hunger and oxygen desaturation if the pneumothorax covers a large area.
- There may be chest pain and a cough with or without hemoptysis.
- No breath sounds are detected over the affected area on auscultation (act of listening to sounds within the human body either directly or using stethoscope or other means).
- A chest x-ray shows air or fluid in the pleural space and reduction in lung volume.
Types of Pneumothorax
- There are various types of pneumothorax. They are as follows:
A) Spontaneous Pneumothorax
- It occurs due to rupture of small blebs (air-filled blisters) that is located on the apex of the lungs.
- These blebs can occur in healthy, young individuals (primary spontaneous pneumothorax) or as a result of various lung diseases such as COPD, asthma, cystic fibrosis, and pneumonia (secondary spontaneous pneumothorax).
- Various factors like smoking, being tall and thin, male gender, family history and previous spontaneous pneumothorax increase the risk of bleb formation.
B) Iatrogenic pneumothorax
- Laceration or puncture of the lung during medical procedures may result to iatrogenic pneumothorax.
- The leading cause of this pneumothorax is transthoracic needle followed by catheter insertion, thoracentesis, pleural biopsy, and transbronchial biopsy.
- Alveoli and bronchioles may rupture from excessive ventilatory pressure during manual or mechanical ventilation called barotrauma.
- Esophageal procedures and tearing during insertion of gastric tube can allow air from the esophagus to enter the mediastinum and the pleural space results in this form of pneumothorax.
C) Traumatic Pneumothorax
- Penetrating (open) or non-penetrating (closed) chest trauma may cause this pneumothorax.
- Air enters the pleural space through an opening in the chest wall that is due to stab or gunshot wounds and surgical thoracotomy which is the result of penetrating trauma.
- A penetrating chest wound may be referred to as a sucking chest wound where during inspiration, air enters the pleural space through the chest wall.
- The wound should be covered with an occlusive dressing that is secured on three sides (vent dressing) in case of emergency treatment.
- During inspiration, as negative pressure is created in the chest, the dressing pulls against the wound that prevents air from entering the pleural space.
- The dressing is pushed out as the pressure rises in the pleural space during expiration which escapes air through the wound and from under the dressing.
- The object responsible for causing the open chest wound should not be removed if it is still in its place until the physician is present.
- A bulky dressing is used to stabilize the impaled object.
- Laceration of the lungs caused by rib fractures can cause air to enter the pleural space in case of non-penetrating chest trauma.
- Alveolar rupture occur secondary to sudden chest compression which is caused by blunt trauma.
D) Tension Pneumothorax
- If air entering the pleural space cannot escape, it results to tension pneumothorax.
- Intra-pleural pressures increasingly elevate if the continued accumulation of air in the pleural space occurs.


- This result in the compression of the lung on the affected side and pressure on the heart and great vessels that pushes them away from the affected side.
- The mediastinum gets shifted towards the unaffected side compressing the “good” lung, which further compromises oxygenation.
- Venous return decreases and cardiac output falls as the pressure increases.
- This pneumothorax may result from either an open or a closed pneumothorax.
- In an open chest wound, a flap may act as a one-way valve due to which air can enter on inspiration but cannot escape.
- Mechanical ventilation and resuscitative efforts can also results in this pneumothorax.
- It also occurs if chest tubes are clamped or become blocked in patient with pneumothorax.
- This situation can be normalized by unclamping the tube or relieving the obstruction.
- This pneumothorax is a medical emergency that affects both respiratory and cardiovascular systems.
- Dyspnea, marked tachycardia, tracheal deviation, decreased or absent breath sounds on the affected side, neck vein distention, cyanosis, and profuse diaphoresis are some of its manifestations.
- The patient is likely to die in this type of pneumothorax from inadequate cardiac output or severe hypoxemia if the tension in the pleural space is not relieved.
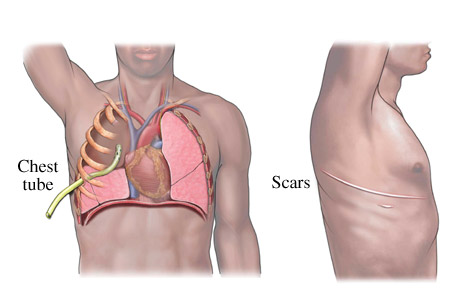
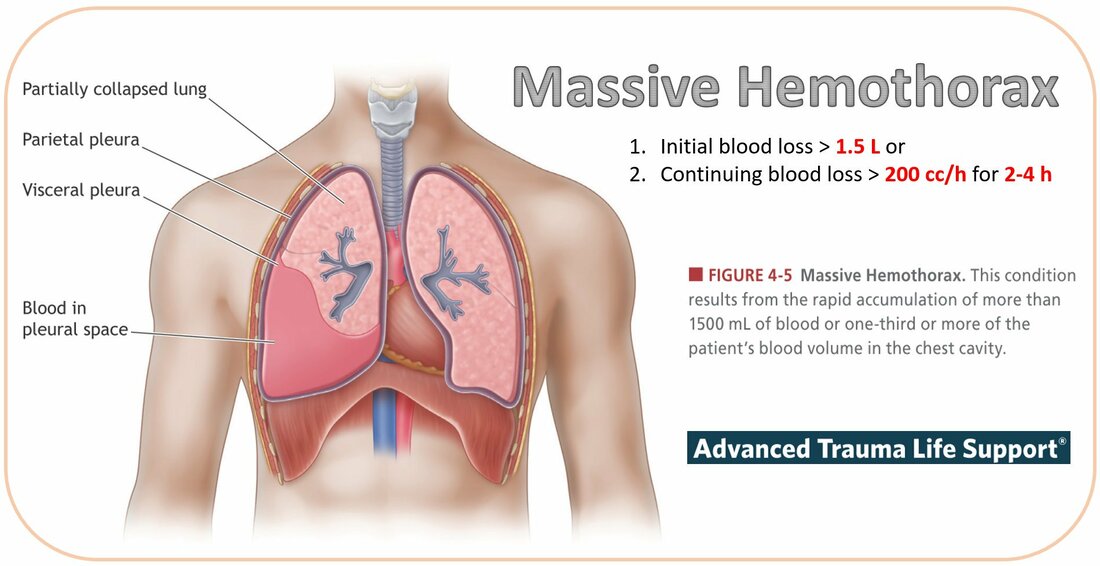
E) Hemothorax
- In this type, blood gets accumulated in the pleural space by various ways like injury to the chest wall, diaphragm, lungs, blood vessels or mediastinum.

- When it occurs with pneumothorax, it is called hemo-pneumothorax.
- Immediate insertion of a chest tube is required in order to evacuate the blood which can be recovered and re-infused for a short time after the injury.
F) Chylothorax
- The presence of lymphatic fluid in the pleural space is called chylothorax.
- The lymphatic fluid fills the pleural space when the thoracic duct is disrupted either traumatically or from a malignancy.
- The lymphatic fluid is milky white and high in lipid content.
- Normal lymphatic flow through thoracic duct is 1500-2500ml/day.
- This amount gets increased by around ten folds after ingestion of fats.
- Conservative treatment like chest drainage, bowel rest and parenteral nutrition can heal 50% of the cases.
- Octreotide has also been used to reduce the flow of lymphatic fluid with some success.
- In case the conservative therapy fails, surgery and pleurodesis can be done.
- Pleurodesis refers to the artificial production of adhesions between the parietal and visceral pleura that is done with a chemical sclerosing agent like talc or doxycycline.
References:
i) https://www.healthline.com/health/collapsed-lung
ii) https://www.medicalnewstoday.com/articles/318110
iii) https://www.physio-pedia.com/Pneumothorax
iv) https://www.webmd.com/lung/what-is-a-collapsed-lung#1