

- Sodium plays a major role being the main cation of extra-cellular fluid (ECF).
- It helps in maintaining the concentration and volume of extra-cellular fluid (ECF) and also influences the water distribution between ECF and intra-cellular fluid (ICF).
- It also helps in the generation and transmission of nerve impulses, muscle contractility and the regulation of acid-base balance.
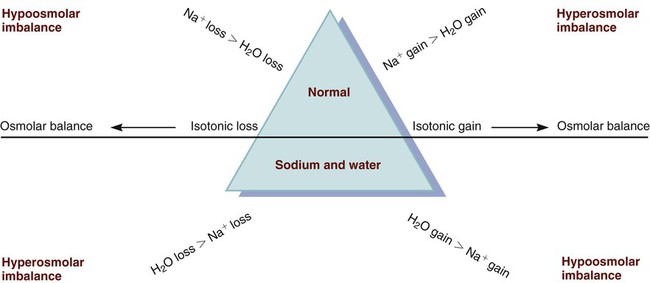
- Sodium is taken as the primary determinant of ECF osmolality so the imbalances of sodium are typically associated with parallel changes in osmolality.
- The serum sodium level reflects the ratio of sodium to water, not necessarily the loss or gain of sodium which is measured in milliequivalents per litre (mEq/L) or millimoles per litre (mmol/L).
- If the sodium level changes in serum, it may reflect a primary water imbalance, a primary sodium imbalance or the combination of the two.
- Thus, sodium imbalances are associated with imbalances in ECF volume.
- Sodium intake is more than its body requirement which is absorbed from foods by the GI tract.
- Sodium leaves the body in various forms like in urine, sweat and feces.
- Kidneys are considered as the primary regulator of sodium balance
- The ECF concentration of sodium is regulated by the kidney in two ways i.e., by excreting or retaining water under the influence of anti-diuretic hormone (ADH).
- Aldosterone is also responsible in regulation of sodium as it promotes sodium re-absorption from the renal tubules.
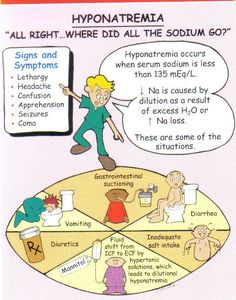

Image source: study
Hypernatremia
- It is the condition when the serum sodium level is elevated either by water loss or by sodium gain.
- It causes hyper-osmolality as sodium is the major determinant of the ECF osmolality and results in ECF hyper-osmolality.
- In turn, there is shifting of water out of the cell which leads to cellular dehydration.
- The primary protection against the development of hyper-osmolality is thirst.
- Hypernatremia is not a big problem for those alert persons who have access to water, can sense thirst, and is able to swallow.
- Impaired level of unconsciousness or an inability to obtain fluids is the results of hypernatremia secondary to water deficiency.
- Hypernatremia is caused by several clinical states from water loss.
- The decrease in the synthesis or release of ADH from the posterior pituitary gland (central diabetes insipidus) and the decreased kidneys response to ADH (nephrogenic diabetes insipidus) can result to profound diuresis which produces a water deficit and hypernatremia.
- Hyper-osmolality with osmotic diuresis can result from the administration of concentrated hyperosmolar tube feedings and hyperglycemia associated with uncontrolled diabetes mellitus.
- Excessive sweating and increased sensible losses from high fever may be the cause of hypernatremia.
- It may also be caused by excessive sodium intake followed by inadequate water intake.
- The various reasons for sodium gain are: IV administration of hypertonic saline or sodium bicarbonate, use of sodium containing drugs, excessive oral intake of sodium (ingestion of seawater) and primary aldosteronism (hyper-secretion of aldosterone) caused by the tumor of the adrenal gland.
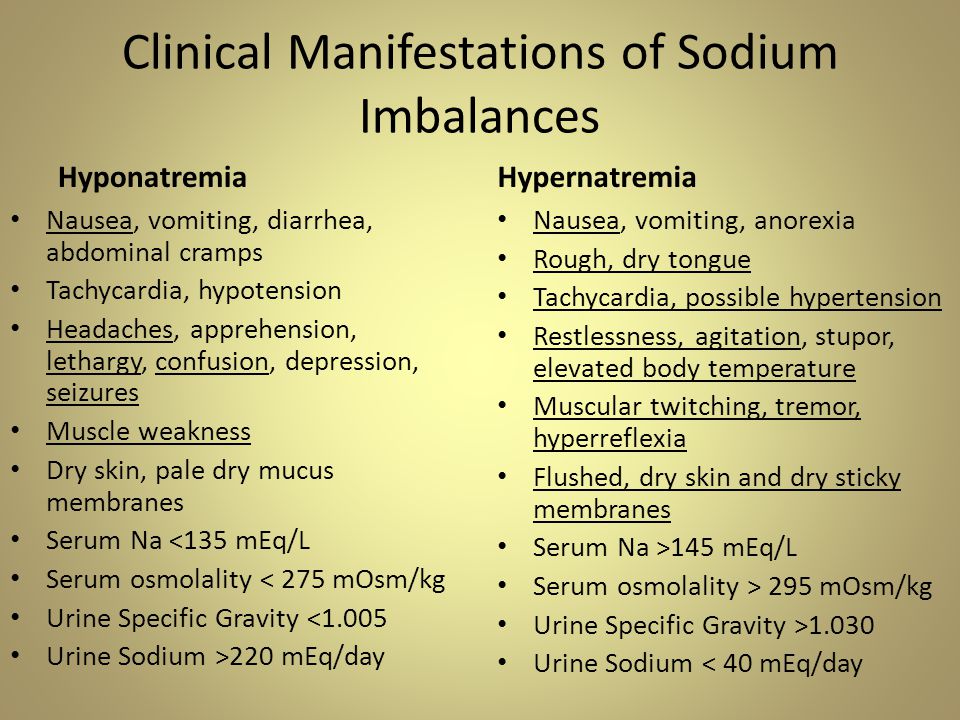
Clinical manifestations of Hypernatremia
- The shifting of water out of the cells into ECF with resultant dehydration and shrinkage of cells are the primary manifestation.
- Dehydration of brain cells results in neurologic manifestations such as intense thirst, agitation, and decreased alertness, ranging from sleepiness to coma.
- Manifestations such as postural hypotension, weakness and decreased skin turgor occur if there is any accompanying ECF volume deficit.
Hyponatremia
- It is the condition when serum sodium level gets decreased as a result of loss of sodium-containing fluids, water excess in relation to the amount of sodium or a combination of both.
- Profuse diaphoresis, draining wounds, excessive diarrhoea or vomiting and trauma with significant blood loss causes loss of sodium which results in hyponatremia.
- Water move towards the cell in response to hypo-osmolality that is the result of hyponatremia.
- Hyponatremia from water excess is also caused by inappropriate use of sodium-free or hypotonic IV fluids which generally occurs in patients after surgery or major trauma or during the administration of fluids in patients with renal failure.
- Excessive water intake is found more in patients with psychiatric disorders.
- Abnormal retention of water causes dilutional hyponatremia which is the result of syndrome of inappropriate antidiuretic hormone secretion (SIADH).

Image source: journalofclinical
Clinical manifestations of Hyponatremia
- Cellular swelling is the result of hyponatremia which is first manifested in the central nervous system.
- Plasma osmolality lowers in response to excess water which shifts fluid into brain cells and causes irritability, headache, confusion, seizures and even coma.
- Irreversible neurologic damage or death may result if severe acute hyponatremia is not treated on time.
References:
i) https://www.jcehepatology.com/article/S0973-6883(21)00244-9/fulltext
iii) https://www.livescience.com/65222-hypernatremia-and-hyponatremia.html