

- Fluid spacing is a term that describes the distribution of water present in a body.
- There are different types of fluid spacing where first spacing means the normal distribution of fluid in ICF (Intra-cellular Fluid) and ECF (Extra-cellular Fluid) compartments.
- Second spacing means an abnormal accumulation of interstitial fluid in body (i.e., edema).
- Third spacing occurs if the fluid that has been accumulated in a portion of body won’t get exchanged with the rest of the ECF.
- The fluid in third spacing becomes unavailable for functional use as it is trapped.

- For examples: ascites, sequestration of fluid in the abdominal cavity with peritonitis and edema associated with burns, trauma or sepsis.
Regulation of Water Balance
- There are various ways by which water present in the body is balanced. Some of the ways are given below:
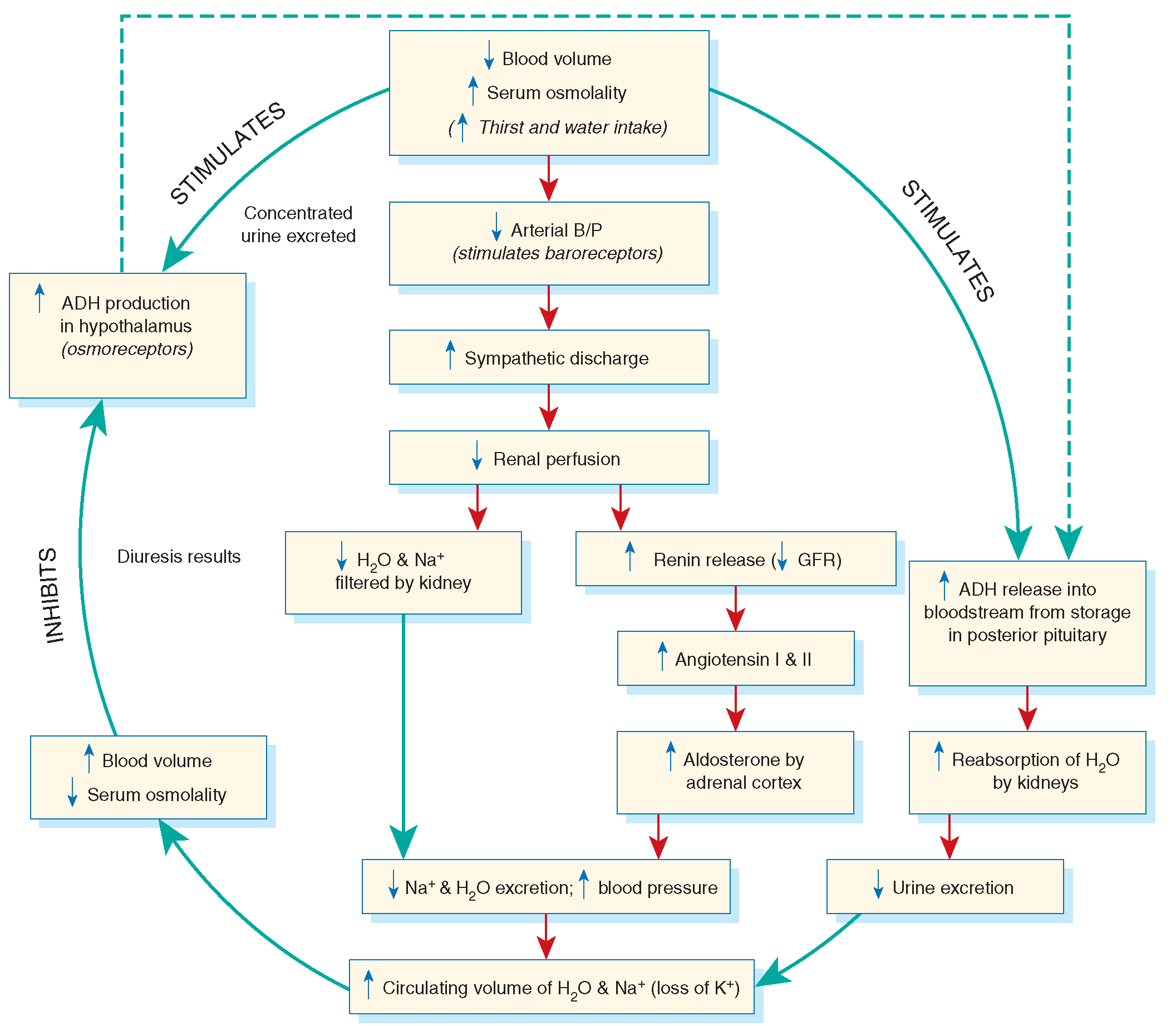
a) Hypothalamic –Pituitary Regulation
- Water balance is maintained via the finely tuned balance of water that is taken and water that is excreted.
- Water ingestion equals water loss in the individual who has free access to water that is by a normal thirst and ADH mechanism and normally functioning kidneys.
- An intact thirst mechanism is critical as it is the primary protection so that development of hyper-osmolality does not occur.
- Osmoreceptors present in the hypothalamus sense a body fluid deficit or increase in the plasma osmolality due to which thirst and ADH release is stimulated.
- Thirst results in intake of water in the patient.
- The distal tubules and collecting ducts in the kidneys respond to ADH by increasing the permeability to water.
- The result is increased in water reabsorption from the tubular filtrate into the blood which decreases excretion of it in the urine.
- Collectively, these factors result in increased free water in body and decreased plasma osmolality.
- The patient is at the risk for fluid deficit and hyperosmolality if he or she cannot recognize or act on the sensation of thirst.
- There are various factors that stimulate ADH release like stress, nausea, nicotine and morphine.
- A decreased plasma osmolality or water excess suppresses secretion of ADH which results in urinary secretion of water.
- It is common for the postoperative patient to have a lower plasma osmolality which may be due to the stress of surgery and opioid analgesia.
- Social and psychologic factors may also affect the desire to consume fluids though they are not related to fluid balance.
- A dry mouth also leads the patient to drink water even there is no water deficit of measurable type.
b) Renal Regulation
- Kidneys are the main (primary) organs for regulating the fluid and electrolyte balance.
- Kidneys adjust urine volume and the urinary excretion of most electrolytes to maintain balance between the overall intake and output.
- The total plasma volume gets filtered several times each day by kidneys.
- In the average adult, the kidney reabsorb 99% of this filtrate which produces around 1.5 litre of urine per day.
- Selective reabsorption of water and electrolytes takes place during the movement of filtrate through the renal tubules and also secretion of electrolytes result in the production of urine that is greatly different in composition and concentration of plasma.
- This process helps in maintaining normal plasma osmolality, electrolyte balance, blood volume and acid-base balance.
- ADH and aldosterone acts on the renal tubules.
- The kidneys fail to maintain fluid and electrolyte balance with severe impaired renal function which results in edema, potassium and phosphorous retention, acidosis, and other electrolyte imbalances.
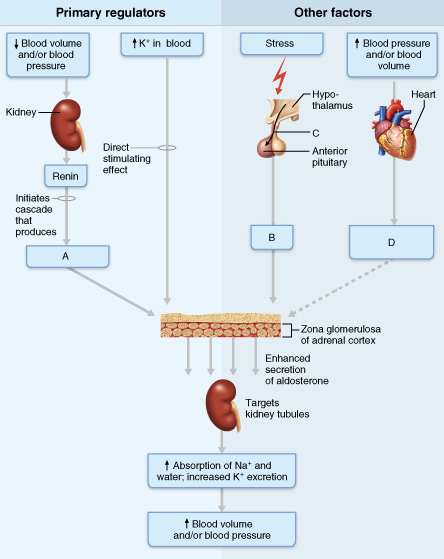
c) Adrenal Cortical Regulation
- Adrenal cortex secretes glucocorticoids and mineralocorticoids that help to regulate both water and electrolytes.
- The glucocorticoids (i.e., cortisol) primarily have an inflammatory effect that results in increase serum glucose levels whereas osmolality, sodium retention and potassium excretion is enhanced by mineralocorticoids i.e., aldosterone.
- When the sodium is reabsorbed, water follows because of osmotic changes.
- Large doses of cortisol function as both glucocorticoids (glucose elevating and anti-inflammatory) and mineralocorticoids (sodium-retention) though it is the most abundant glucocorticoids.
- Normally cortisol secretion is in a diurnal or circadian pattern.
- If cortisol secretion is increased in response to physical and psychologic stress, it affects many body functions including fluid and electrolyte balance.
- Aldosterone has sodium retention and potassium excreting capabilities as it is a mineralocorticoids.
- Aldosterone secretion occurs when there is decreased renal perfusion or decreased sodium delivery to the distal portion of renal tubule.
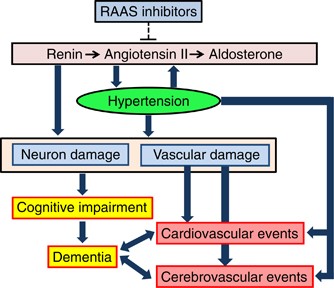
- This decrease activates the renin-angiotensisn-aldosterone system (RAAS) which results in secretion of aldosterone.
- The secretion of aldosterone is also stimulated by increased plasma potassium, decreased plasma sodium, and adrenocorticotropic hormone from the anterior pituitary acting directly on the adrenal cortex.
d) Cardiac regulation
- Cardiomyocytes produce hormones like natriuretic peptides i.e., atrial natriuretic peptide (ANP) and b-type natriuretic peptide (BNP) which are natural antagonists to RAAS system.
- They are produced when atrial pressure (increased volume, such as occurs in heart failure) increases and also when serum sodium levels is high.
- Their secretion suppresses the secretion of aldosterone, renin, and ADH and also the function of angiotensin II.
- In the renal tubules, these peptides promote excretion of sodium and water which decreases blood volume and blood pressure.
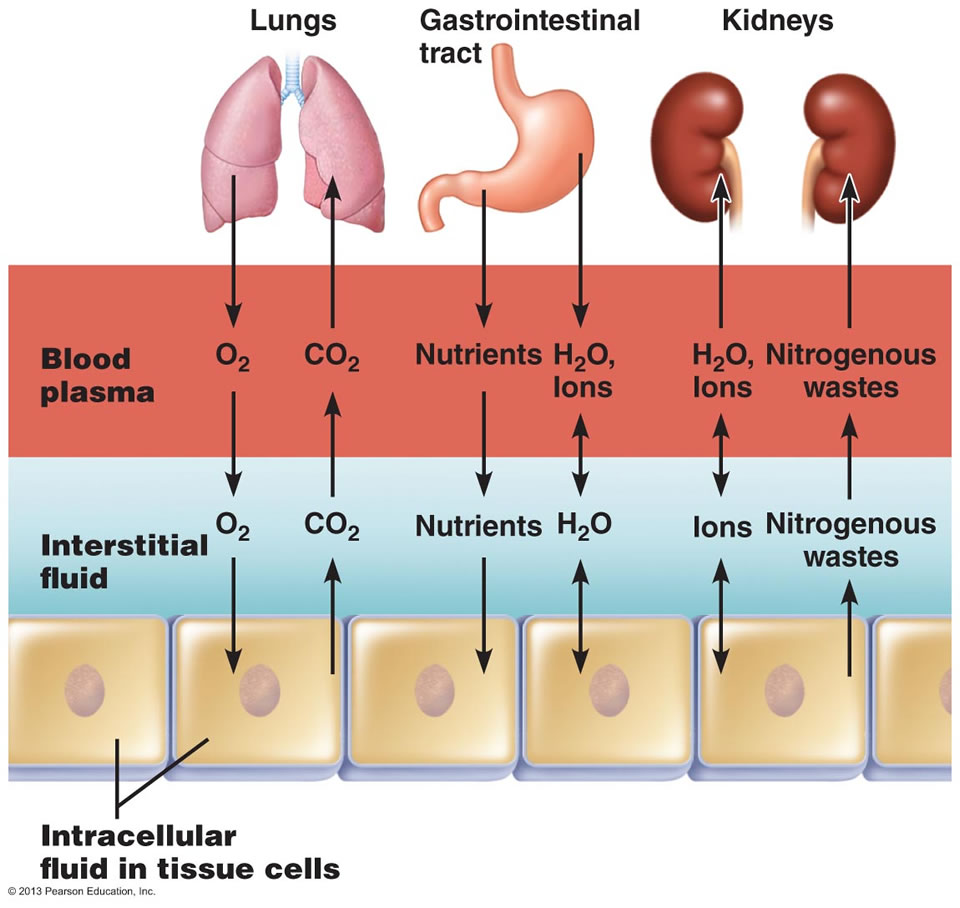
e) Gastrointestinal Regulation
- Daily water intake and output are normally between 2000 and 3000 ml.
- Oral intake of fluids accounts for the most of the intake of water.
- Water from food metabolism and water present in solid foods also adds in water intake.
- Lean meat is approximately 70% water whereas the water content of fruits and vegetables is almost 100%.
- Beside oral intake, GI tract also secretes around 8000ml of digestive fluids each day which is reabsorbed in the GI tract of which only a small amount is released in feces.
- Diarrhea and vomiting can lead to significant fluid and electrolyte loss which hampers the GI reabsorption of this secreted fluid.
f) Insensible water loss
- Invisible vaporization from the lungs and skin that assists in regulating body temperature is known as insensible water loss which ranges from 600-900 ml/day.
- Water loss also increases with the accelerated body metabolism which occurs with increased body temperature and exercise.
- There may be confusion about water loss through skin in the form of sweat from sweat glands.
- But only sensible perspiration (excessive sweating) caused by exercise, fever or high environmental temperatures may lead to large loss of water and electrolytes.
References:
i) https://pubmed.ncbi.nlm.nih.gov/1342242/
ii) https://sperimentando.com/?p=1474
iii) https://wtcs.pressbooks.pub/nursingfundamentals/chapter/15-2-basic-fluid-and-electrolyte-concepts/
iv) https://open.oregonstate.education/aandp/chapter/26-1-body-fluids-and-fluid-compartments/